
Nocardia asteroides is an aerobic, gram-positive, partially acid-fast, filamentous bacterium that belongs to the order Actinomycetales. While not typically considered part of the normal human microbiome, N. asteroides is an environmentally ubiquitous organism found in soil, decaying vegetation, and water. It can cause opportunistic infections in humans, particularly in those with compromised immune systems.
Key Characteristics
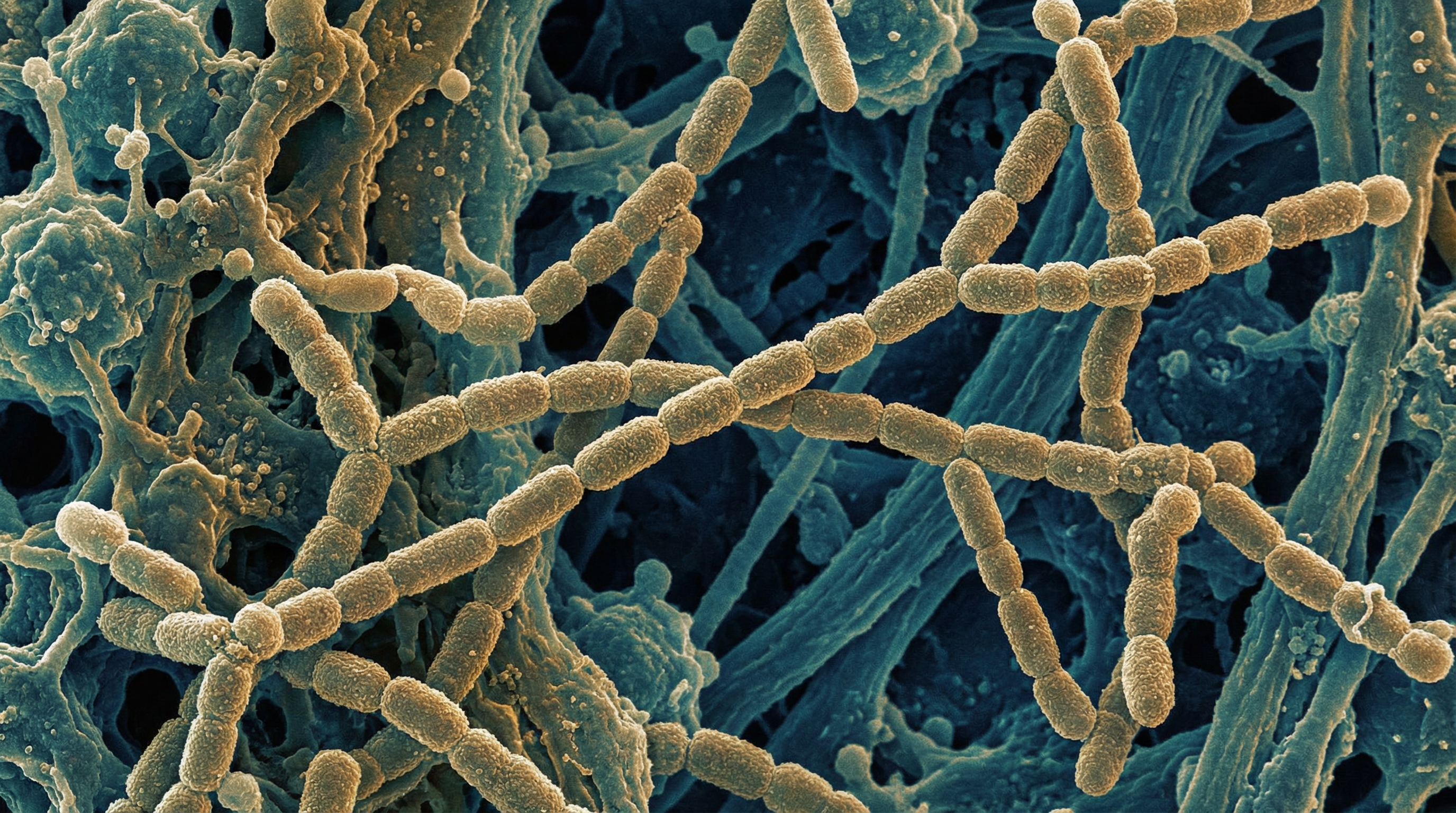
N. asteroides is characterized by its branching, filamentous morphology that can fragment into rod-shaped or coccoid elements. It is aerobic, catalase-positive, and partially acid-fast, meaning it retains certain acid-fast dyes but less strongly than Mycobacteria. The bacterium grows slowly in culture, typically requiring 3-5 days for visible colonies to appear, which are often described as having a chalky white or orange appearance with a powdery surface.
N. asteroides is part of the "Nocardia asteroides complex," which includes several closely related species that have been reclassified over time with advances in molecular identification techniques. This complex is responsible for the majority of human Nocardia infections, with N. asteroides being the most frequently isolated species.
Relationship to Human Health
Unlike many bacteria covered in this database, N. asteroides is not considered a normal resident of the human microbiome. Instead, it is an environmental organism that can cause opportunistic infections when introduced into the human body, particularly in individuals with impaired immunity.
Pulmonary Nocardiosis
The most common manifestation of N. asteroides infection is pulmonary nocardiosis, which occurs when the bacterium is inhaled from the environment. Clinical features include:
- Chronic cough, often productive with purulent sputum
- Fever and night sweats
- Chest pain
- Weight loss
- Fatigue
- Dyspnea (shortness of breath)
Radiographic findings in pulmonary nocardiosis are variable and non-specific, including nodules (which may cavitate), infiltrates, pleural effusions, and abscesses. This variability often leads to delayed diagnosis, as the presentation can mimic tuberculosis, fungal infections, or lung malignancies.
Disseminated Nocardiosis
From the lungs, N. asteroides can disseminate hematogenously to virtually any organ system, with the central nervous system being a particularly common site of secondary infection. Approximately 44% of patients with systemic nocardiosis develop CNS involvement, typically presenting as brain abscesses. Other sites of dissemination include:
- Skin and soft tissues
- Kidneys
- Joints
- Bones
- Heart
- Eyes
Primary Cutaneous Nocardiosis
Though less common than pulmonary infection, N. asteroides can cause primary cutaneous nocardiosis following traumatic inoculation of the organism through the skin. This can manifest as:
- Cellulitis
- Subcutaneous abscesses
- Lymphocutaneous syndrome (similar to sporotrichosis)
- Mycetoma (chronic granulomatous infection with sinus tract formation)
Risk Factors for Infection
N. asteroides primarily affects individuals with compromised immune systems. Major risk factors include:
- Corticosteroid therapy
- Organ transplantation
- HIV/AIDS
- Malignancies, particularly hematologic cancers
- Chronic lung diseases such as chronic obstructive pulmonary disease (COPD)
- Diabetes mellitus
- Alcoholism
- Autoimmune disorders requiring immunosuppressive therapy
However, approximately 10-15% of nocardiosis cases occur in apparently immunocompetent individuals, suggesting that other factors may influence susceptibility to infection.
Diagnosis and Identification
Diagnosing N. asteroides infection is challenging due to its non-specific clinical presentation and the difficulty in isolating the organism. Diagnostic approaches include:
- Direct microscopy of clinical specimens (sputum, abscess drainage, tissue biopsy) using Gram stain and modified acid-fast stains
- Culture on appropriate media, with extended incubation periods (up to 2-3 weeks)
- Molecular methods such as PCR and 16S rRNA gene sequencing for species identification
- Imaging studies (CT, MRI) to assess the extent of infection, particularly in suspected disseminated cases
All patients diagnosed with nocardiosis should undergo brain imaging to rule out CNS involvement, even in the absence of neurological symptoms.
Treatment Approaches
Treatment of N. asteroides infection typically involves:
- Long-term antibiotic therapy (often 6-12 months)
- Trimethoprim-sulfamethoxazole (TMP-SMX) as the first-line agent
- Alternative or additional antibiotics may include amikacin, imipenem, ceftriaxone, minocycline, or linezolid
- Surgical drainage of abscesses when appropriate
- Reduction of immunosuppressive therapy when possible
Antibiotic susceptibility testing is crucial, as resistance patterns vary among Nocardia species and strains. Treatment regimens often need to be tailored based on susceptibility results and the site and severity of infection.
Interaction with the Human Microbiome
As an environmental organism rather than a normal constituent of the human microbiome, N. asteroides' interactions with the resident microbiota are not well characterized. However, several observations are noteworthy:
- The healthy respiratory microbiome may provide colonization resistance against Nocardia through competition for nutrients and space
- Disruption of the normal respiratory microbiota by broad-spectrum antibiotics or underlying lung disease may create niches that facilitate Nocardia colonization
- The immunomodulatory effects of the gut microbiome may influence systemic immune responses to Nocardia infection
Research Challenges and Future Directions
Research on N. asteroides faces several challenges:
- The relatively low incidence of nocardiosis limits large-scale clinical studies
- The slow growth of the organism complicates laboratory investigations
- Taxonomic revisions within the Nocardia genus have led to inconsistencies in the literature
Future research directions include:
- Improved rapid diagnostic methods to facilitate earlier detection and treatment
- Better understanding of virulence factors and pathogenesis
- Investigation of potential interactions between Nocardia and the resident microbiota
- Development of more effective and targeted antimicrobial therapies
- Exploration of host genetic factors that may influence susceptibility to nocardiosis